Abstract
In this study, a novel contact tracing model that leverages smartphone technology to enhance efficiency, reduce costs, and extend the duration of contact tracing efforts is developed. This model utilizes smartphones as identification systems, collecting data on the proximity of other smartphone users through integrated Bluetooth and GPS technology. The study examines the frequency, duration, and proximity of interactions between smartphone devices in a clinical setting, highlighting potential implications for infectious disease transmission to pilot the mobile application developed. Contact data from six pairs of devices were analyzed, focusing on metrics such as total contacts, total contact time, average contact time, average distance, and the percentage of contacts occurring within 1.5 meters. The results showed varying levels of interaction across device pairs, with Devices 1 & 3 showing the highest number of contacts (175), and Devices 3 & 4 displaying the longest average contact time (20,133,193.01 seconds). Correlation analysis revealed weak and statistically insignificant relationships between total contacts and average distance (r = 0.13, p = 0.81), contact time and the percentage of close contacts (r = -0.15, p = 0.78). These findings suggest that while there are observable trends in contact patterns, the statistical insignificance highlights the need for further investigation to establish stronger associations that could inform infection control practices in healthcare settings.
Keywords
Contact Tracing, Smartphone Technology, Bluetooth and GPS, Infectious Disease Transmission, Correlation Analysis
1. Background
The coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
| [1] | World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it; 2020. Available from: https://tinyurl.com/t82w9ka |
[1]
. This infectious respiratory disease was first detected in Wuhan City, China, in December 2019. It was declared a global pandemic by the World Health Organization (WHO) on 11 March, 2020 and has infected over two million people worldwide and over 150,000 people have lost their lives to this respiratory disease
| [2] | Ekong I, Chukwu E, Chukwu M. COVID-19 Mobile Positioning Data Contact Tracing and Patient Privacy Regulations: Exploratory Search of Global Response Strategies and the Use of Digital Tools in Nigeria. JMIR Mhealth Uhealth 2020; 8(4): e19139. https://doi.org/10.2196/19139 |
[2]
. The first case of COVID-19 was reported in Nigeria on 27 February 2020 in an Italian man who returned to Ogun state and transferred to a hospital in Lagos
| [3] | Nigeria Centre for Disease Control. COVID-19 outbreak in Nigeria: Situation report (116); 2020. |
[3]
. By 10 July, 2020, 30,748 cases of COVID-19 had been reported across 35 of 36 states in Nigeria and the Federal Capital Territory
. This was a drastic increase since the index case was reported on 27 February, 2020. To better manage the spread, Nigeria’s Federal Government declared a lockdown in key affected states including Lagos, Ogun, and the Federal Capital Territory. The lockdown was in addition to several mitigating actions taken by state governments such as the ban on social gatherings and dusk-to-dawn curfews. Nigeria, the most populous country in Africa, had also been impacted by the outbreak, with over 266,000 confirmed cases and more than 3,000 deaths as of 19 July 2023
.
COVID-19 ravaged the Nigerian economy and disrupted the lives of its citizens, and as such intensive efforts were put in place by the Federal Government to stem the rise of the pandemic. The efforts involved utilizing contact tracing to find individuals who might have come in contact with an identified symptomatic patient, through information provided by the symptomatic individual, which may be biased and provide a stemmed contact tracing model which may not capture possible infected persons. Different strategies were adopted by governments around the world to track and isolate COVID-19 patients and their contacts and/ or for lockdown or lock-in enforcement. The state of Massachusetts in the United States announced the launch of its first contact tracing call center to be manned by 1000 virtual assistants
while China used a mandatory smartphone app “Health code” that leverages a mesh network for infected persons contact tracing and notification
. Italy, Germany, and Austria
adopted strategies in which telecommunications providers allowed for the sharing of location data with health authorities to check whether people stayed at home. The data was aggregated and anonymous, mapping concentrations rather than individuals to respect Europe’s privacy laws. Singapore used a mobile app that uses a Bluetooth-based mesh network to detect people's proximity to those who had been exposed to COVID-19 and warned them to get tested if they come in close contact with the infected
. The Nigeria Centre for Disease Control (NCDC) has been reported to conduct contact tracing of over 9000 contacts of confirmed cases to effectively contain the spread of COVID-19, in line with the recommended measures for pandemic response
| [12] | Bell D, Nicoll A, Fukuda K, Horby P, Monto A, et al. Non-pharmaceutical interventions for pandemic influenza, national and community measures. World Health Organization Writing Group; Emerg Infect Dis; 2006. https://doi.org/10.3201/eid1201.051371 |
| [13] | Luca F, Chris W, Michelle K, Lele Z, Anel Nurtay et al. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science; 2020. |
[12, 13]
. These measures included antiviral, vaccine, and nonpharmaceutical measures such as case isolation, household quarantine, school or workplace closure, and travel restrictions among others. Although, the nonpharmaceutical measures had been the only practical option in the absence of any known antiviral drug, these measures require enormous resources considering the experience of the countries (Italy, United Kingdom, China and the United States) despite their advanced health care systems. It was certain at that time that the number of confirmed cases were under reported in Nigeria and most African countries
| [2] | Ekong I, Chukwu E, Chukwu M. COVID-19 Mobile Positioning Data Contact Tracing and Patient Privacy Regulations: Exploratory Search of Global Response Strategies and the Use of Digital Tools in Nigeria. JMIR Mhealth Uhealth 2020; 8(4): e19139. https://doi.org/10.2196/19139 |
[2]
and this was a bad omen for Africa if isolation, containment, quarantine, and contact-tracing mechanisms were not properly implemented then as the pandemic had exposed the weak health care systems in Nigeria. One effective and complementary strategy to mitigate the spread and reduce the impact of infectious disease like COVID-19 is to trace the primary and secondary contacts of confirmed cases using a cost-effective digital contact tracing model.
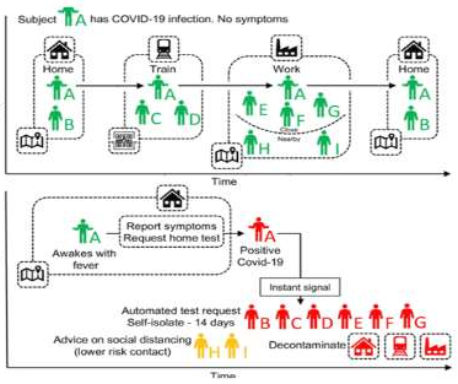
Therefore, a more robust contact tracing model that embraces technology, minimizes contact tracing cost and maximizes contact tracing time is proposed in this study. The model uses a smartphone that acts as an identification system, gathering information concerning smartphone owner and the other smartphone owners within proximity via GPS. This solution is built around Bluetooth and GPS technology. The diagram in
Figure 1 illustrates the proposed method in this study. The coronavirus disease (COVID-19) pandemic adversely affected the global economy and the health of the people. Its adverse effects are still evolving, with deaths estimated to reach over 40 million globally
. The fundamental reason behind this study is that the digital contact tracing model utilizes mobile technology which is a brilliant idea since mobile phone ownership has grown rapidly over the years. O’Dea
affirmed there is an active mobile phone subscription of around 140 million against about 200 million Nigerians, (about 75%)
. This therefore serves as the basis for building a novel model that utilizes mobile technology as an effective contact-tracing solution. Smartphones could generate complex strings of characters and exchange them, providing a way to know whether people have been near each other without the need for personal information.
The adoption of digital solutions in Nigeria has been focused on electronic forms for contact data collection and visualization for follow-up
. Digital technologies can do more than a tool for field data collection or serve as an outbreak investigation platform
| [19] | Islam, M. Extensively Drug-Resistant Tuberculosis in the Time of COVID-19—How has the Landscape Changed for Pakistan? Disaster Medicine and Public Health Preparedness. 2020; 14(4). https://doi.org/10.1017/dmp.2020.230 |
[19]
. This contact tracing modelling approach is novel and innovative in Nigeria and Africa at large as each installation of the app would have a single universally unique identifier (UUID) and no personal information (Name, Date of birth, Email address) would be harvested and the privacy of all the participants will be protected. The app would also require high-level access to Bluetooth information from the device, specifically the device’s Media Access Control (MAC) address and the MAC address of nearby devices (the device in question would be forced to broadcast its MAC). Another innovation is that the application would provide the participant with a key code in order to seed the UUID upon installation. The participants can supply a private key/password/biometric so that the UUID can be revoked at any time by the participants and the respective UUID acts as the public key. This model may require additional datasets such as location-aware call descriptor records with suitably hashed subscriber attributes subject to regulatory approval. This contact tracing method can also be used in monitoring and controlling the spread of other infectious diseases such as Tuberculosis (TB), Multi-Drug Resistant TB (MDRTB) and Ebola among other infectious diseases. Our healthcare system suffered a setback due to the effects of COVID-19 and as a result conditions of patients with TB and MDRTB were worse and transmission of such infectious diseases was high at that period
| [20] | Hasan T, Nguyen VN, Nguyen HB, Nguyen TA, Le HTT, Pham CD, et al. Retrospective Cohort Study of Effects of the COVID-19 Pandemic on Tuberculosis Notifications, Vietnam, 2020. Emerg Infect Dis. 2022; 28(3): 684-92. https://doi.org/10.3201/eid2803.211919 |
| [21] | Migliori GB, Visca D, van den Boom M, Tiberi S, Silva DR, Centis R, et al. Tuberculosis, COVID-19 and hospital admission: consensus on pros and cons based on a review of the evidence. Pulmonology. 2021; 27(3): 248-56. https://doi.org/10.1016/j.pulmoe.2020.12.016 |
| [22] | Suresh K. S., Shiv K. M., Kalpana T. and Rakhi G. How to cal-culate sample size for observational and experimental nursing research studies? National Journal of Physiology, Pharmacy and Pharmacology 2020; 10 (1), 1-8. https://doi.org/10.5455/njppp.2020.10.0930717102019 |
[20-22]
. The goal of this study is to develop a robust digital contact tracing model application and present its use on smartphones to improve testing capacity and control the spread of COVID-19 and other infectious diseases. The aim was achieved by generating a universally unique identifier (UUID) for each of the participants using the mobile application developed. The UUID information from other participants will then be collected at proximity and forwarded to the server (local server developed for a pilot study) for system wide-analysis. Due to the fact that by the time the App was developed the number of persons testing for COVID-19 had decreased drastically, the App was piloted among six TB patients attending the DOTS centre at the Nigerian Institute of Medical Research. Hence the app has the advantage of being used for other infectious diseases and not restricted to Coronavirus 2019 disease.
2. Methodology
2.1. Study Setting
This study was conducted at the Nigerian Institute of Medical Research (NIMR). Nigerian Institute of Medical Research is the foremost medical research institute in the country, an agency of the Federal Ministry of Health and one of the designated centres for SARS-COV-2 testing. The institute is located in Lagos Mainland and easily accessible from all parts of the state. This centre tests not less than 400 (80 participants per day) patients weekly. The modified drive-through centre for SARS-COV-2 testing was initially proposed to be used for the pilot study since it caters for people who reside in Lagos and across the country and as one of the key affected states in Nigeria. However, due to the fact that by the time the App was developed, the number of individuals for COVID-19 test had reduced drastically hence the App was piloted among patients attending the DOTS centre of NIMR.
2.2. Study Design
The study adopted a prospective cohort study design that employs a digital-based technology. The GPS tracked a nearby participant when the mobile app was turned on, the participant’s phone used radio waves to figure out which other devices were nearby. In this case, it would blast out an opaque string of characters called an identifier beacon and other nearby phones would make a time-stamped log of that identifier. The beacon would change every few minutes to prevent location tracking and because it would be a random string of characters, the beacon would mean nothing to anyone even if they could see it. The result is that, on each phone with the app, there would be an anonymous record going back 14 days of which other phones have been in close proximity. Each participant will be followed up daily for 14 days from the last point of exposure. The study linked the contact as well as followed them up through the incubation period.
2.3. Study Population
This included participant aged 18 years and above attending DOTS Centre in NIMR and who had previously tested positive for Tuberculosis (TB) and on DOTS.
2.4. Inclusion and Exclusion Criteria
Participants between 18 years and above who have previously tested positive for TB and are willing to participate in the study. Participants with a smart phone were included in the study. Participants without a smartphone were not included in the study.
2.5. Sample Size Determination
The minimum number of the sample size for the study was calculated using a single proportion formula
:
where n is the sample size, z is the selected critical value of desired confidence level for a two-tailed test and it is equal to 1.96, p is the estimated prevalence set at 2%
| [24] | Yasaka T. M., Lehrich B. M., Sahyouni R. Peer-to-Peer Contact Tracing: Development of a Privacy Preserving Smartphone App. JMIR Mhealth Uhealth 2020; 8(4): e18936 https://doi.org/10.2196/18936 |
[24]
and d is the desired level of precision given by 5%. The required minimum sample size for this study was initially estimated to 50 participants, who have not been previously tested for SARS-COV-2 with the assumption that participants would be readily available for SARS-COV-2 testing. Though, it has been documented that projection of at least three cases can lead to thousands of contacts. However, this study used six TB patients attending the DOTS centre at the Nigerian Institute of Medical Research for piloting the use of the app. The TB patients were used since COVID-19 pandemic has drastically reduced and people coming for SARS-Cov-2 testing were not easily found at the time of concluding the contact tracing mobile app development.
2.6. Sampling Method
The selection of the participants was based on systematic random sampling method. Participants coming into DOTS centre at the Nigerian Institute of Medical Research were systematically selected.
2.7. Study Procedure
2.7.1. Architecture
The mobile app solution developed was based on Bluetooth and GPS technology to detect participant's proximity to those who have been exposed to TB and warn them to get tested if they come in close contact via text messages. The app was developed following the scenario shown in
Figure 2.
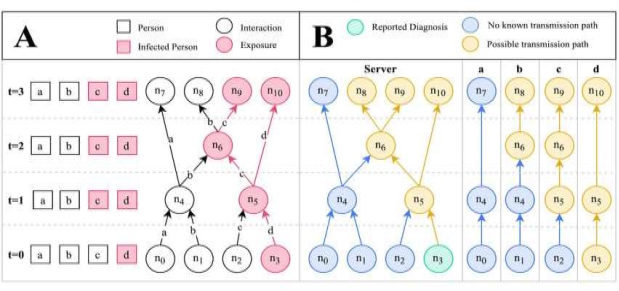
Figure 2. Disease spread scenario modelled as a transmission graph.
The A is the graphical representation of a disease spread scenario across time. Contact points with infected individuals are denoted as exposures. Uninfected individuals may become infected at exposure points according to some probability (the transmission rate); hence, b does not become infected at n
6. The B is the transmission graph corresponding to the scenario in A, depicting the information that is available to the server and each individual's smartphone app. Only one node, n
3, is associated with a reported diagnosis. The infection risk level at the other contact points can be inferred by checking for possible transmission paths, n: node and t: time point
| [25] | Olsen M., Lohning A., Campos M., Jones P., McKirdy S., Alghafri R., et al., Mobile phones of paediatric hospital staff are never cleaned and commonly used in toilets with implications for healthcare nosocomial diseases, Sci. Rep. 11(1), 12999; 2021. https://doi.org/10.1038/s41598-021-92360-3 |
[25]
. The proposed contact tracing technique for infectious diseases is the first of its kind in Nigeria and Africa to the best of our knowledge.
2.7.2. How the Smartphones use Bluetooth and GPS Technology for Contact Tracing
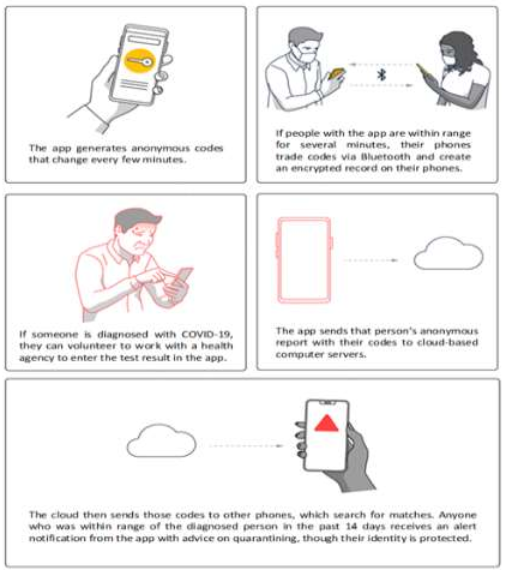
The smartphone generated complex strings of characters and exchange them, providing a way to know those participants have been near each other without the need for personal information (
Figure 3).
Figure 3. Utilizing Bluetooth and GPS technology in contact tracing.
The developed application was tested for one week, looking at the different steps of data collection before the actual study. Feedbacks and trouble-shooting were utilized to help improve and smoothen the process of the pilot study.
2.8. Alpha and Beta Versions of the Novel Contact Tracing Mobile Application
The proposed contact tracing mobile app was designed in two different versions to ensure that it reaches its highest potential and is perfect for the purpose it is meant for. The Alpha and Beta models determined the right mobile app to use at the end of the design. The mobile app was therefore developed and tested in Alpha and Beta versions before the pilot phase. The errors detected in the Alpha version of the app were fixed and improved upon to have the Beta version.
Figure 4. Final version of the Contact Tracing Mobile Application Developed.
2.9. Data Collection
A questionnaire was designed to collect social demographic data and confirm use and acceptability of the app and information on contact details was collected via a Bluetooth and GPS-based mobile app developed. Data collectors were adequately trained for a period of five days on the study instrument in order to effectively installed the app and collect data from the participants.
2.10. Data Management and Analysis
Data obtained from the study were stored on a laptop used as a local server or data centre. Only the mobile phone numbers of participants served as the identifier needed to run the application which were kept confidential and only known to the research team and strictly used for the purpose of the study. The phone numbers became necessary for follow – up of the infective.
The Haversine formula calculates the distance between two points on the surface of a sphere given their longitudes and latitudes.
The Haversine formula is given as:
Where:
and are the latitudes of device 1 and device 2 in radians.
is the difference between the latitudes of device 1 and device 2 in radians.
is the difference between the longitudes of device 1 and device 2 in radians.
r is the radius of the Earth (mean radius = 6,371 km)
Python was used to develop the contact tracing mobile application and analyses that generated data points, including the device ID, latitude, longitude, date, and time for multiple devices as shown in the results section were generated using the same software.
3. Ethical Consideration
Ethical approval was obtained from the Nigerian Institute of Medical Research (NIMR) Institutional Review Board (IRB) with ethical code IRB/20/093. The prospective participants were duly informed of their rights to either participate or not and to withdraw at any time. All the participants were required to sign a consent form of participation in the research.
4. Results
The distance between two locations given the latitude and longitude obtained from the app for the two devices in meters was calculated using the Haversine formula.
Table 1. Summary of Device Contacts and Distances for Infectious Disease Safety Considerations.
Pair | Total Contacts | Total Contact Time (s) | Avg Contact Time (s) | Avg Distance (m) | % Contacts < 1.5 m |
Device 1 & 2 | 127 | 523447454 | 4121633.50 | 5170.60 | 2.36 |
Device 1 & 3 | 175 | 545934942 | 3119628.24 | 5984.75 | 2.29 |
Device 1 & 4 | 104 | 451251074 | 4338952.63 | 4079.92 | 0.96 |
Device 2 & 3 | 175 | 546387533 | 3122214.47 | 7317.69 | 0.57 |
Device 2 & 4 | 80 | 333785525 | 4172319.06 | 4529.87 | 3.75 |
Device 3 & 4 | 113 | 2275050810 | 20133193.01 | 12489.87 | 1.77 |
The total number of contacts shown in
Table 1 represented the frequency of interactions between the devices which also showed the frequency of close interactions between the two participants involved. High contact frequencies indicated increased opportunities for transmission of infectious diseases.
For instance, the interaction between Device 1 and Device 3 (175 total contacts) suggested a higher risk of potential exposure compared to Device 2 and Device 4 (80 total contacts). This finding could inform guidelines on limiting the frequency of close interactions to reduce transmission risks, especially in high-contact areas like emergency rooms or TB clinics.
Total Contact Time measures the cumulative duration of all contacts in seconds. Extended contact times could heighten the risk of disease transmission, as longer interactions might facilitate the spread of infectious diseases, especially those transmitted via respiratory droplets or surface contact.
For instance, Device 3 and Device 4 recorded the highest total contact time (2,275,050,810 seconds), which might indicate a prolonged exposure period. This could be relevant for procedures requiring prolonged patient contact, such as during surgeries or intensive care monitoring, where enhanced protective measures should be considered. The average contact time also provided details into the typical duration of each interaction. Longer average contact times could suggest scenarios where participants remain for extended period of time, increasing the risk of transmission.
The average contact time for Device 3 and Device 4 (20,133,193.01 seconds) was significantly higher than the others. This suggests the need for careful monitoring and possibly stricter infection control protocols during prolonged interactions, such as during procedures that involve close patient monitoring or extended care.
Average Distance indicated the typical distance between devices during contacts. Larger distances generally correlate with lower transmission risks, while shorter distances (e.g., <1.5 m) are associated with higher transmission potential, particularly for airborne pathogens. The relatively small average distance between Device 1 and Device 4 (4,079.92 meters) suggests a closer interaction compared to Device 3 and Device 4 (12,489.87 meters). A close proximity could necessitate the use of personal protective equipment (PPE) or physical barriers to mitigate transmission risks.
The percentage of contacts within 1.5 meters is a critical measure for assessing the risk of transmission, as this distance is often considered a threshold for close contact transmission of infectious diseases like COVID-19. For Device 2 and Device 4, 3.75% of contacts were within 1.5 meters, which is the highest among the pairs. This might indicate a need for stricter controls in environments where close interactions were more frequent, such as ensuring adequate distancing measures, enhancing ventilation, or implementing regular disinfection protocols.
Table 2. Correlation Analysis of Contact Metrics and Proximity Indicators for Infectious Disease Safety.
| Correlation Coefficient (r) | P-value |
Total Contacts vs. Average Distance | 0.13 | 0.81 |
Contact Time vs. % Contacts < 1.5 m | -0.15 | 0.78 |
The correlation analysis revealed a weak positive relationship between total contacts and average distance, with a correlation coefficient (r) of 0.13. This shows that as the number of contacts increases, the average distance between contacts slightly increases. However, the p-value of 0.81 indicates that this relationship is not statistically significant, meaning the observed correlation could likely be due to chance. Similarly, the correlation between contact time and the percentage of contacts occurring at distances less than 1.5 meters was weakly negative, with r-value of -0.15. This indicates that as contact time increases, the percentage of close contacts (less than 1.5 meters) tends to decrease slightly. However, the p-value of 0.78 suggests that this relationship is also not statistically significant, indicating that the data do not provide strong evidence of a meaningful association between these variables.
5. Discussion of Findings
The results obtained through the pilot study of the contact tracing mobile application developed provide insights into the potential risks of infectious disease transmission based on device interactions in clinical settings
| [26] | Lindsley J. A., Reynolds C. D., Williams T., Underwood J., Ingram A. N., Jowitt J., et al., How dirty is your phone? Evaluating restroom behavior and cell phone surface contamination, Joint Comm. J. Qual. Patient Saf. 46 (10) 588–590; 2020. https://doi.org/10.1016/j.jcjq.2020.06.008 |
| [27] | Chao Foong Y., Green M., Zargari A., Siddique R., Tan V., Brain T., et al., Mobile phones as a potential vehicle of infection in a hospital setting, J. Occup. Environ. Hyg. 12 (10) D232–D235; 2015. https://doi.org/10.1080/15459624.2015.1060330 |
| [28] | Kirkland K. B., Weinstein J. M. Adverse effects of contact isolation. Lancet. 1999 Oct 2; 354(9185): 1177-8. https://doi.org/10.1016/S0140-6736(99)04196-3 |
[26-28]
. The high frequency of contacts between certain devices, such as Device 1 and Device 3 (175 contacts), underscores the increased likelihood of transmission opportunities in scenarios where devices or individuals frequently interact. This is particularly relevant in high-contact areas like emergency rooms or clinics specializing in infectious diseases, where limiting the frequency of close interactions may be necessary to reduce transmission risks
| [29] | Evans H. L., Shaffer M. M., Hughes M. G., Smith R. L., Chong T. W., Raymond D. P., Pelletier S. J., Pruett T. L., Sawyer R. G. Contact isolation in surgical patients: a barrier to care? Surgery. 2003 Aug; 134(2): 180-8. https://doi.org/10.1067/msy.2003.222 |
| [30] | Delgado-Rodríguez M, Bueno-Cavanillas A, López-Gigosos R, de Dios Luna-Castillo J, Guillén-Solvas J, Moreno-Abril O, Rodríguez-Tuñas B, Cueto-Espinar A, Rodríguez-Contreras R, Gálvez-Vargas R, et al. Hospital stay length as an effect modifier of other risk factors for nosocomial infection. Eur J Epidemiol. 1990 Mar; 6(1): 34-9. https://doi.org/10.1007/BF00155546 |
[29, 30]
.
Moreover, the total contact time is a critical factor in assessing exposure risks. For instance, the extended contact time observed between Device 3 and Device 4 (2,275,050,810 seconds) indicates prolonged exposure periods that could significantly increase the likelihood of disease transmission, particularly for pathogens spread via respiratory droplets or through direct contact. This finding is particularly important for clinical procedures that require prolonged patient interaction, such as surgeries or intensive care, where enhanced protective measures, such as the use of personal protective equipment (PPE), are essential
| [31] | Tess BH, Glenister HM, Rodrigues LC, Wagner MB. Incidence of hospital-acquired infection and length of hospital stay. Eur J Clin Microbiol Infect Dis. 1993 Feb; 12(2): 81-6. https://doi.org/10.1007/BF01967579 |
| [32] | Leung, N. H. L., Chu, D. K. W., Shiu, E. Y. C., Chan, K., McDevitt, J. J., Hau, B. J. P. et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nature Medicine; 2020, 26, 676-680. https://doi.org/10.1038/s41591-020-0843-2 |
[31, 32]
.
The average distance between interacting devices further informs transmission risk, with shorter distances generally correlating with higher transmission potential. The relatively small average distance between Device 1 and Device 4 (4,079.92 meters) suggests closer interactions, which may necessitate the implementation of physical barriers or stricter PPE usage to mitigate transmission risks. The percentage of contacts occurring within 1.5 meters is particularly of concern, given the established risk of airborne transmission within this range. The finding that 3.75% of interactions between Device 2 and Device 4 occurred within this proximity stresses the need for stringent infection control measures, especially in environments where close contact is unavoidable. This could include enforcing physical distancing, improving ventilation, and regular disinfection of surfaces, particularly in high-risk areas.
6. Conclusion
A contact tracing mobile application has been developed in this study to generate a universally unique identifier (UUID) for each of the participants and collect a UUID information from other participants via their smartphones. The use of this app will help track individuals who are in close contact with people who tested positive, for immediate isolation, testing and control the spread of infectious diseases.
The findings through the pilot study conducted using the contact tracing mobile application emphasize the importance of monitoring and controlling interactions between the participants to mitigate the risk of infectious disease transmission in clinical and healthcare settings. Although the observed correlations between contact metrics and proximity indicators were weak and statistically insignificant, the data still suggest areas where infection control practices could be improved, particularly in high-contact and prolonged interaction scenarios. Further research with a larger sample size and more comprehensive data collection is necessary to strengthen the evidence base and refine guidelines for minimizing transmission risks in healthcare environments.
Abbreviations
COVID-19 | Coronavirus Disease 2019 |
App | Application |
NCDC | Nigeria Centre for Disease Control |
UUID | Universally Unique Identifier |
MAC | Media Access Control |
TB | Tuberculosis |
MDRTB | Multi-Drug Resistant Tuberculosis |
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it; 2020. Available from:
https://tinyurl.com/t82w9ka
|
| [2] |
Ekong I, Chukwu E, Chukwu M. COVID-19 Mobile Positioning Data Contact Tracing and Patient Privacy Regulations: Exploratory Search of Global Response Strategies and the Use of Digital Tools in Nigeria. JMIR Mhealth Uhealth 2020; 8(4): e19139.
https://doi.org/10.2196/19139
|
| [3] |
Nigeria Centre for Disease Control. COVID-19 outbreak in Nigeria: Situation report (116); 2020.
|
| [4] |
Roser R., Ritchie, H., Ortiz-Ospina, E. and Hasell, J. “Nigeria: Coronavirus Pandemic Country Profile,” Our World in Data, 2023. [Online]. Available:
https://ourworldindata.org/coronavirus/country/nigeria
[Accessed: 03- Aug- 2023].
|
| [5] |
Carraggi MP. MA to launch first coronavirus contact tracing program in US; 2020. Available from:
https://patch.com/massachusetts/boston/ma-launch-first-coronavirus-contacttracingprogram-u-s
|
| [6] |
Rafalski EM. Health insurance portability and accountability Act of 1996 (HIPAA). Encyclopedia of Health Services Research 1996.
https://doi.org/10.4135/9781412971942.n180
|
| [7] |
Zhang O. Inside China's smartphone 'health code' system ruling post-coronavirus life; 2020. Associated Press/Time: Available from:
https://time.com/5814724/china-health-codesmartphones-coronavirus/
|
| [8] |
Pollina E, Busvine D. European mobile operators share data for coronavirus fight. Reuters; 2020. Available from:
https://tinyurl.com/yadpu9gm
|
| [9] |
Choudhury SR. Singapore says it will make its contact tracing tech freely available to developers. CNBC; 2020. Available from:
https://www.cnbc.com/2020/03/25/coronavirussingapore-to -make-contact -tracing-tech-open-source.html
|
| [10] |
Woods A. CDC to launch new surveillance system to track coronavirus spread. New York Post; 2020. Available from:
https://nypost.com/2020/03/26/cdc-to-launch-new-surveillancesystem-to-track-coronavirus-spread/
|
| [11] |
World Health Organization. 2020 Apr 03. Coronavirus disease 2019 (COVID-19): Situation Report - 74 URL:
https://www.who.int/docs/default-source/coronaviruse/situationreports/20200403-sitrep-74-covid-19-mp.pdf?sfvrsn=4e043d03_12
[accessed 2020-08-29]
|
| [12] |
Bell D, Nicoll A, Fukuda K, Horby P, Monto A, et al. Non-pharmaceutical interventions for pandemic influenza, national and community measures. World Health Organization Writing Group; Emerg Infect Dis; 2006.
https://doi.org/10.3201/eid1201.051371
|
| [13] |
Luca F, Chris W, Michelle K, Lele Z, Anel Nurtay et al. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science; 2020.
|
| [14] |
Van Elsland SL, O'Hare R. Coronavirus pandemic could have caused 40 million deaths if left unchecked: Imperial College London; 2020. Available from:
https://www.imperial.ac.uk/news/196496/coronavirus-pandemic-could-have-caused-40/
|
| [15] |
Statista; 27 2020. Available from:
https://www.statista.com/statistics/467187/forecast-ofsmartphone-users-innigeria/#:~:text=There%20are%20around%20170%20million,population%20is%20using%20a%20smartphone.&text=Smartphone%20penetration%20is%20set%20to,phone%20and%20smartphone%20manufacturers%20alike
|
| [16] |
Dimagi.com. Digital solution for COVID-19 response; 2020. Available from:
https://www.dimagi.com/covid-19/
|
| [17] |
Robin Muccari. NBC News, Apple/ Google; 2020. Available from:
https://www.nbcnews.com/news/obituaries/coronavirus-deaths-60-stories-victims-aroundcountry-n1194396
|
| [18] |
Shibasaki R. International Telecommunication Union. 2017. [2020-03-20]. Call detail record (CDR) analysis: Sierra Leone
https://www.itu.int/en/ITU-D/Emergency-Telecommunications/Documents/2017/Reports/SL/D012A0000CA3301PDFE.pdf
|
| [19] |
Islam, M. Extensively Drug-Resistant Tuberculosis in the Time of COVID-19—How has the Landscape Changed for Pakistan? Disaster Medicine and Public Health Preparedness. 2020; 14(4).
https://doi.org/10.1017/dmp.2020.230
|
| [20] |
Hasan T, Nguyen VN, Nguyen HB, Nguyen TA, Le HTT, Pham CD, et al. Retrospective Cohort Study of Effects of the COVID-19 Pandemic on Tuberculosis Notifications, Vietnam, 2020. Emerg Infect Dis. 2022; 28(3): 684-92.
https://doi.org/10.3201/eid2803.211919
|
| [21] |
Migliori GB, Visca D, van den Boom M, Tiberi S, Silva DR, Centis R, et al. Tuberculosis, COVID-19 and hospital admission: consensus on pros and cons based on a review of the evidence. Pulmonology. 2021; 27(3): 248-56.
https://doi.org/10.1016/j.pulmoe.2020.12.016
|
| [22] |
Suresh K. S., Shiv K. M., Kalpana T. and Rakhi G. How to cal-culate sample size for observational and experimental nursing research studies? National Journal of Physiology, Pharmacy and Pharmacology 2020; 10 (1), 1-8.
https://doi.org/10.5455/njppp.2020.10.0930717102019
|
| [23] |
Almagor, J., Picascia, S. Exploring the effectiveness of a COVID-19 contact tracing app using an agent-based model. Sci Rep 10, 22235 (2020).
https://doi.org/10.1038/s41598-020-79000-y
|
| [24] |
Yasaka T. M., Lehrich B. M., Sahyouni R. Peer-to-Peer Contact Tracing: Development of a Privacy Preserving Smartphone App. JMIR Mhealth Uhealth 2020; 8(4): e18936
https://doi.org/10.2196/18936
|
| [25] |
Olsen M., Lohning A., Campos M., Jones P., McKirdy S., Alghafri R., et al., Mobile phones of paediatric hospital staff are never cleaned and commonly used in toilets with implications for healthcare nosocomial diseases, Sci. Rep. 11(1), 12999; 2021.
https://doi.org/10.1038/s41598-021-92360-3
|
| [26] |
Lindsley J. A., Reynolds C. D., Williams T., Underwood J., Ingram A. N., Jowitt J., et al., How dirty is your phone? Evaluating restroom behavior and cell phone surface contamination, Joint Comm. J. Qual. Patient Saf. 46 (10) 588–590; 2020.
https://doi.org/10.1016/j.jcjq.2020.06.008
|
| [27] |
Chao Foong Y., Green M., Zargari A., Siddique R., Tan V., Brain T., et al., Mobile phones as a potential vehicle of infection in a hospital setting, J. Occup. Environ. Hyg. 12 (10) D232–D235; 2015.
https://doi.org/10.1080/15459624.2015.1060330
|
| [28] |
Kirkland K. B., Weinstein J. M. Adverse effects of contact isolation. Lancet. 1999 Oct 2; 354(9185): 1177-8.
https://doi.org/10.1016/S0140-6736(99)04196-3
|
| [29] |
Evans H. L., Shaffer M. M., Hughes M. G., Smith R. L., Chong T. W., Raymond D. P., Pelletier S. J., Pruett T. L., Sawyer R. G. Contact isolation in surgical patients: a barrier to care? Surgery. 2003 Aug; 134(2): 180-8.
https://doi.org/10.1067/msy.2003.222
|
| [30] |
Delgado-Rodríguez M, Bueno-Cavanillas A, López-Gigosos R, de Dios Luna-Castillo J, Guillén-Solvas J, Moreno-Abril O, Rodríguez-Tuñas B, Cueto-Espinar A, Rodríguez-Contreras R, Gálvez-Vargas R, et al. Hospital stay length as an effect modifier of other risk factors for nosocomial infection. Eur J Epidemiol. 1990 Mar; 6(1): 34-9.
https://doi.org/10.1007/BF00155546
|
| [31] |
Tess BH, Glenister HM, Rodrigues LC, Wagner MB. Incidence of hospital-acquired infection and length of hospital stay. Eur J Clin Microbiol Infect Dis. 1993 Feb; 12(2): 81-6.
https://doi.org/10.1007/BF01967579
|
| [32] |
Leung, N. H. L., Chu, D. K. W., Shiu, E. Y. C., Chan, K., McDevitt, J. J., Hau, B. J. P. et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nature Medicine; 2020, 26, 676-680.
https://doi.org/10.1038/s41591-020-0843-2
|
Cite This Article
-
APA Style
Musa, A. Z., Osuolale, K. A., Salako, A. O., Ifeta, A. T., Salako, B. L. (2024). Developing a Novel Contact Tracing Mobile Application for Coronavirus Disease 2019 (COVID-19) for Improving Testing Capacity and Controlling the Spread of COVID-19 in Nigeria. Science Journal of Public Health, 12(5), 169-177. https://doi.org/10.11648/j.sjph.20241205.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Musa, A. Z.; Osuolale, K. A.; Salako, A. O.; Ifeta, A. T.; Salako, B. L. Developing a Novel Contact Tracing Mobile Application for Coronavirus Disease 2019 (COVID-19) for Improving Testing Capacity and Controlling the Spread of COVID-19 in Nigeria. Sci. J. Public Health 2024, 12(5), 169-177. doi: 10.11648/j.sjph.20241205.13
Copy
|
Download
AMA Style
Musa AZ, Osuolale KA, Salako AO, Ifeta AT, Salako BL. Developing a Novel Contact Tracing Mobile Application for Coronavirus Disease 2019 (COVID-19) for Improving Testing Capacity and Controlling the Spread of COVID-19 in Nigeria. Sci J Public Health. 2024;12(5):169-177. doi: 10.11648/j.sjph.20241205.13
Copy
|
Download
-
@article{10.11648/j.sjph.20241205.13,
author = {Adesola Zaidat Musa and Kazeem Adewale Osuolale and Abideen Olurotimi Salako and Adekunle Temu Ifeta and Babatunde Lawal Salako},
title = {Developing a Novel Contact Tracing Mobile Application for Coronavirus Disease 2019 (COVID-19) for Improving Testing Capacity and Controlling the Spread of COVID-19 in Nigeria
},
journal = {Science Journal of Public Health},
volume = {12},
number = {5},
pages = {169-177},
doi = {10.11648/j.sjph.20241205.13},
url = {https://doi.org/10.11648/j.sjph.20241205.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20241205.13},
abstract = {In this study, a novel contact tracing model that leverages smartphone technology to enhance efficiency, reduce costs, and extend the duration of contact tracing efforts is developed. This model utilizes smartphones as identification systems, collecting data on the proximity of other smartphone users through integrated Bluetooth and GPS technology. The study examines the frequency, duration, and proximity of interactions between smartphone devices in a clinical setting, highlighting potential implications for infectious disease transmission to pilot the mobile application developed. Contact data from six pairs of devices were analyzed, focusing on metrics such as total contacts, total contact time, average contact time, average distance, and the percentage of contacts occurring within 1.5 meters. The results showed varying levels of interaction across device pairs, with Devices 1 & 3 showing the highest number of contacts (175), and Devices 3 & 4 displaying the longest average contact time (20,133,193.01 seconds). Correlation analysis revealed weak and statistically insignificant relationships between total contacts and average distance (r = 0.13, p = 0.81), contact time and the percentage of close contacts (r = -0.15, p = 0.78). These findings suggest that while there are observable trends in contact patterns, the statistical insignificance highlights the need for further investigation to establish stronger associations that could inform infection control practices in healthcare settings.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Developing a Novel Contact Tracing Mobile Application for Coronavirus Disease 2019 (COVID-19) for Improving Testing Capacity and Controlling the Spread of COVID-19 in Nigeria
AU - Adesola Zaidat Musa
AU - Kazeem Adewale Osuolale
AU - Abideen Olurotimi Salako
AU - Adekunle Temu Ifeta
AU - Babatunde Lawal Salako
Y1 - 2024/10/18
PY - 2024
N1 - https://doi.org/10.11648/j.sjph.20241205.13
DO - 10.11648/j.sjph.20241205.13
T2 - Science Journal of Public Health
JF - Science Journal of Public Health
JO - Science Journal of Public Health
SP - 169
EP - 177
PB - Science Publishing Group
SN - 2328-7950
UR - https://doi.org/10.11648/j.sjph.20241205.13
AB - In this study, a novel contact tracing model that leverages smartphone technology to enhance efficiency, reduce costs, and extend the duration of contact tracing efforts is developed. This model utilizes smartphones as identification systems, collecting data on the proximity of other smartphone users through integrated Bluetooth and GPS technology. The study examines the frequency, duration, and proximity of interactions between smartphone devices in a clinical setting, highlighting potential implications for infectious disease transmission to pilot the mobile application developed. Contact data from six pairs of devices were analyzed, focusing on metrics such as total contacts, total contact time, average contact time, average distance, and the percentage of contacts occurring within 1.5 meters. The results showed varying levels of interaction across device pairs, with Devices 1 & 3 showing the highest number of contacts (175), and Devices 3 & 4 displaying the longest average contact time (20,133,193.01 seconds). Correlation analysis revealed weak and statistically insignificant relationships between total contacts and average distance (r = 0.13, p = 0.81), contact time and the percentage of close contacts (r = -0.15, p = 0.78). These findings suggest that while there are observable trends in contact patterns, the statistical insignificance highlights the need for further investigation to establish stronger associations that could inform infection control practices in healthcare settings.
VL - 12
IS - 5
ER -
Copy
|
Download